Displaying items by tag: medical impact
Consider Joining the Abortion Pill Rescue Network!
 |
 |
Christian was rescued from a chemical abortion in 2016.
What should a woman do if she starts a chemical abortion and has regrets?
A woman who would like to learn more about reversing the effects of chemical abortion and possibly continuing her pregnancy should call the Abortion Pill Reversal (APR) hotline at 877-558-0333 or go to the APR website to begin a live chat. The Abortion Pill Rescue Network™ (APRN) has nurses waiting to answer questions, explain reversal, and connect her with an APR provider in her area.
How does a medical professional enroll in the Abortion Pill Rescue Network?
Healthcare professionals with prescribing privileges can go to our provider website, click Join Our Medical Network, and specify that you would like to "provide progesterone treatment.” After receiving the information, we will confirm eligibility and add the medical provider and/or clinic to the APR Provider list. This list is used by our nurses when a client in your area requests a reversal.
We will also send you the APR Kit, which includes a program description, protocol, and documents used throughout the reversal process as well as several research articles.
How do Pregnancy Help Organizations enroll in the Abortion Pill Rescue Network?
A Pregnancy Help Medical Clinic (PHMC) offering APR services provides progesterone by dispensing onsite or through a prescription, confirming the viability and dating of the pregnancy with ultrasound, and the prescribing physician sees the patient (either at the center or in his/her office), ideally within 72 hours.
The other option for centers is to become a "consulting" center. These centers educate and refer for APR and offer free ultrasounds. They seek funding for clients in their community who cannot pay for the progesterone prescription or appointment. And they offer pregnancy and community support for women who have attempted reversal. This is the link to enroll as an APR provider or consulting center.
For more information about APRN, please contact us at info@apr.life.

APRN Medical Director, Dr. Brent Boles, and APRN Advisory Team: Dr. Matt Harrison, Dr. George Delgado, Dr. William Lile, Dr. Julie McDonald, Dr. Karen Poehailos and Dr. Catherine Stark.
Pre-Abortion Screening in Pregnancy Help Medical Clinics
by Christa Brown, Senior Director, Medical Impact, Heartbeat International
As the U.S. Food and Drug Administration (FDA) continues to relax safety measures for mifepristone/misoprostol abortion, the abortion industry shrugs off any responsibility for their part in creating significant hazards to women's health. Despite significant evidence of risk, the FDA continues to modify the Risk Evaluation and Mitigation Strategy (REMS) safety net for mifepristone. Currently, chemical abortion may be administered without a physical exam or ultrasound to confirm the location and age of the pregnancy, Rhesus antigen (Rh) status testing, or any interaction with a medical professional. The American Association of Prolife Obstetricians and Gynecologists (AAPLOG) cautions that “removing all testing recommendations (previously considered standard of care) is such a new approach that studies do not exist to demonstrate the full range of adverse events” that will soon present themselves and that “…complications will undoubtedly be higher.” Big Abortion continues to demonstrate that abortion at all costs, as well as higher profit margins, are the priority as they further distance themselves from real healthcare.
The abortion pill may be dispensed at a clinic or through a telehealth visit, which is completed by phone or video chat. Chemical abortion is also available on more than 70 websites and several funnel abortion services to areas they deem are underserved—delivering directly to the woman’s doorstep. According to the Abortion Pill Rescue® Network, the number of women obtaining the abortion pill online or from a friend has increased tenfold in the last three years.
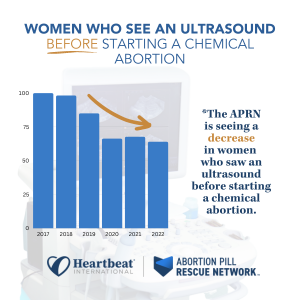
At the Abortion Pill Rescue Network (APRN), we've sadly seen a reduction in pre-abortion exams or ultrasounds before the start of their abortions. These are the percentages of women who called the APR Hotline who received an ultrasound before starting an abortion from 2017-2022:
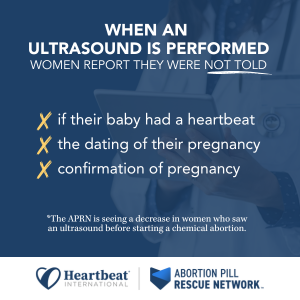
Even when an ultrasound is performed, many women share with APRN nurses that they were not provided the vital information from the scan and do not know if their babies had a heartbeat, the dating of the pregnancy, or if the pregnancy was confirmed to be intrauterine. Because of the failure of the FDA to protect women, there is a gap in information, care, and resources for those considering all options in pregnancy.
Who can be assisted through Pre-Abortion Screening in a pregnancy help medical clinic?
Typically, these appointments are helpful for those who are:
- considering all options for their pregnancies
- scheduling an abortion appointment at an abortion facility, or
- ordering the abortion pill by mail or telehealth
Pregnancy help medical clinics (PHMCs) are in a unique position to offer no-cost medical assessments, safety plans and personal support. Offering a pre-abortion screening is one way to empower women with information about the details of their pregnancies and the choices available to them.
What services are typically included in a pre-abortion screening?
Each center serves its unique community and tailors their services to the needs of the families they serve. Many centers are already offering pre-abortion screenings and have shared that this service is nothing new–just a combination of what they have been doing all along. These clinics offer more choices than abortion facilities and provide concrete solutions to help families overcome barriers to healthy pregnancies.
Care Without Coercion or Cost
PHMCs want families to focus on their own needs, not on how they will pay for care or support. Unlike abortion facilities, PHMCs offer all services without cost to the client. The pre-abortion assessment is an opportunity for a woman considering choices to obtain a free consultation with a licensed healthcare professional who will provide evidence-based information about all her options. Since many women are prescribed the abortion pill with little or no interaction with a healthcare professional, there is immense value in this visit. The PHMC healthcare professional will take the time to answer all the patient’s questions and ensure she makes an informed choice; patients are not pressed to decide for the sake of quick profit.
Confirmation of Pregnancy with A Medical Grade Test
Pregnancy testing is performed by medical professionals, and the results are provided to the patient during the appointment. There are two types of pregnancy tests: a urine sample, and a blood sample. Both pregnancy test types detect the presence of a hormone called human chorionic gonadotropin (hCG). When the preborn baby is implanted in a woman’s uterine lining, hCG hormones begin to develop and multiply. This is a presumptive sign of pregnancy and the PHMC can confirm the patient’s home test results.
Ultrasound Exam for Viability, Dating, And Placement of Pregnancy
AAPLOG recommends an “ultrasound and exam before medication abortion to confirm gestational age” and that “[to] evaluate for ectopic pregnancy [is] important to maternal safety.” They also confirm that informed consent is a professional obligation, and it would be impossible to tailor counseling about chemical abortion to each patient if an ultrasound were not performed.
Some states require women to have an ultrasound exam before an abortion, but these are becoming fewer and fewer. The frequency of ultrasound by abortion providers decreased during the pandemic when “no touch abortions” were advertised. Now those who sell abortion through telehealth or websites have profited from this omission. However, ultrasound is a common service of PHMCs.
The need for an ultrasound before an abortion is threefold:
- Viability
Mayo Clinic estimates that about 10 to 20 percent of known pregnancies end in miscarriage but states the actual number is likely higher because many miscarriages occur very early in pregnancy. If the baby does not have a heartbeat, there is no need for an abortion. Instead, if the pregnancy is not viable, the patient would be referred to her obstetrician for treatment. - Dating
The American College of Obstetricians and Gynecologists (ACOG) points to research that shows how inaccurate LMP (last menstrual period) dating is, reporting that “in about 40% of pregnancies the LMP is not known or information is not reliable." Accurate confirmation of gestational age with ultrasound measurement reduces the potential for taking medication abortion pills outside of the recommended window. The FDA has approved mifepristone through 10 weeks of pregnancy. Higher gestational age is associated with higher failure rates of medication abortion with failure rates rising after week eight, approaching 7% at 10 weeks, and reaching 40% in the second trimester. - Placement
The FDA warns that a contraindication of mifepristone is a suspected ectopic pregnancy or undiagnosed adnexal mass. Mayo Clinic recommends a transvaginal ultrasound to reveal the exact location of the pregnancy. Women have mistakenly assumed they had an intrauterine pregnancy and attempted, unsuccessfully, to chemically abort. A PHMC can determine if the patient has an intrauterine or ectopic pregnancy.
Blood Type/Rh Factor Testing
The ACOG recommends that “Rh D immune globulin be given to Rh-negative women having any type of abortion.” Yet one-third of Americans do not know their blood type so it would be challenging to do this without testing. The AAPLOG recommends that “all pregnant women undergoing medication abortion or otherwise should be evaluated for Rh status.” PHMCs can offer this simple testing to protect women and future pregnancies from complications.
Mayo Clinic explains that risk occurs when even a small amount of the baby's blood could come in contact with the mother’s blood. This can happen if there is bleeding during pregnancy, such as during a chemical abortion, but can be prevented by Rh testing early in pregnancy.
Health problems usually do not occur during a Rh-negative woman’s first pregnancy with a Rh-positive baby. This is because her body does not have a chance to develop a lot of antibodies. The AAPLOG warns that ignoring these recommendations to test pregnant women before abortion may have significant consequences for future pregnancies.
Rh factor is typically determined with a complete panel during an early prenatal visit but can be performed with a fingerstick using a blood-typing kit in a PHMC.
Hemoglobin Testing
Chemical abortion can cause a significant amount of bleeding and sometimes even hemorrhaging. This extra blood loss increases the risk of blood transfusion for those who are anemic. The Cleveland Clinic explains that iron deficiency is common in pregnancy. The chances of needing a blood transfusion after an abortion are increased if the patient is already anemic.
Anemia during pregnancy, defined as hemoglobin (Hb) < 10.5–11 g/dL, is experienced by as many as 40% of women. Anemia following pregnancy is associated with an increased risk for blood transfusion, postpartum depression, and increased mortality.
The World Health Organization estimates that approximately 27% of maternal deaths are due to obstetric hemorrhages.
Typically a simple fingertip prick can determine iron levels which can be performed in a PHMC setting.
STD Testing
The Centers for Disease Control estimates that one in five people (more than 26 million) in the United States have a sexually transmitted disease. According to the National Library of Medicine, pelvic infection is the most common complication of abortion, and the presence of an existing lower genital tract infection increases the risk of complications. According to this study, women seeking abortion “are at significant risk of harboring sexually transmitted diseases (STDs)” and, when combined with an abortion, can lead to long-term pelvic pain and fertility issues. Since STDs can be asymptomatic, women can reduce their risk of complications after an abortion by testing and obtaining treatment before starting an abortion.
Many centers already offer this service and can include this as part of their pre-abortion screening.
Reversal of Mifepristone (Abortion Pill Reversal™) Information
All women considering abortion should know that their options do not end when they consume the first chemical in an abortion. The possibility exists that she can continue her pregnancy if she has regret after taking mifepristone and help is available 24 hours a day to do so. Abortion pill reversal has a nearly 70% success rate and APRN data shows that more than 4,500 lives have been saved through the APRN. No woman should be forced to complete an abortion she no longer desires, and she must be aware of this possibility before the start of the abortion so she can seek reversal treatment as soon as possible.
Safety Plan Information
Chemical abortion is always self-managed, typically in the home of the patient. Yet abortion with mifepristone and misoprostol has four times the complications of surgical abortion. Patients must determine when bleeding or pain requires urgent medical attention, and oftentimes women are alone in the process. While privacy and the comfort of home might sound appealing as she makes an abortion choice, it can be alarming when emergency care is needed. Before consuming the abortion pill, patients need to consider:
- Who will be present during the abortion process?
- How and where will help be sought in a medical emergency?
- When is urgent care required?
The patient and support person should have a plan for when to obtain urgent care in the days after the abortion. She should seek medical attention right away if she has:
- a fever of 100.4°F or higher that lasts for more than four hours
- severe abdominal pain
- heavy bleeding (soaking through two thick, full-size sanitary pads per hour for two hours in a row), or
- stomach pain or discomfort including weakness, nausea, vomiting, or diarrhea, for more than 24 hours after taking misoprostol
 Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
At the emergency department, the patient must explain what medications she has consumed and her precise symptoms. If available, the FDA advises the patient to take the Medication Guide for Mifeprex when seeking medical care so that it can be readily understood that she is undergoing a chemical abortion.
A follow-up plan should be made with a trusted healthcare provider about 7 to 14 days after taking the abortion pills to be sure that the abortion is complete and there are no complications that could lead to infection and hemorrhage. PHMCs have referrals for trusted obstetricians in their communities that can ensure the well-being of these patients following an abortion.
Why are PHMCs the place for pre-abortion screenings?
In every pregnancy, there are two patients: two lives, two heartbeats, and two sets of DNAs. Pre-abortion screening enables PHMCs to care for and protect both patients.
PHMCs advocate for women, not just before the choice is made but afterward, too. Sometimes the answers are not a “quick fix,” and the road to a pregnancy decision may require time and tangible assistance. PHMCs ensure the long-term well-being of their patients and their children and understand that the answer to an unexpected pregnancy is not a “quick fix” that the abortion industry promotes.
___________________________________________________________________________________________________________________________
If your center wants assistance or has questions regarding these services, please contact our Medical Impact team at medical@heartbeatinternational.org.